
Mulu’s History
Mulu arrived at Gambo Hospital emergency department with severe stiffness.
It was stabilized, resuscitated and initiated intravenous antibiotics after performing lumbar puncture.
Within a few days of treatment, Mulu had not only returned to her normal tone, but was also running around the hospital. The intravenous antibiotic creates a miraculous change in a matter of days; in its absence, she will be dead.
#meningitis #worldmeningitisday #meningitissurvivor#defeatmeningitis #defeatmeningitis2030 #Africa#Ethiopia#healthcare #healthworkers
#meningitis #worldmeningitisday #meningitissurvivor#defeatmeningitis #defeatmeningitis2030 #Africa #Ethiopia#healthcare #healthworkers


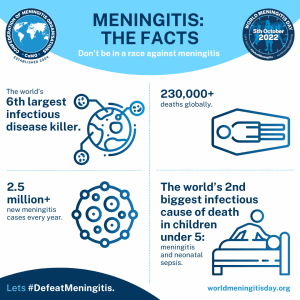
World Meningitis Day is on the 5th of October
and we were delighted to be joined by millions of people around the world to raise awareness of meningitis, a disease that can tragically take a life in under 24 hours. The campaign date is different from previous years; you can read our official announcement explaining why this year is different here.
We look forward to commemorating the next World Meningitis Day with you all on 5th October, 2022! If you can’t wait and want to get involved in the fight to defeat meningitis now, learn more about how to become a memberor feel free to contact us at info@comomeningitis.org.
- Claim: Out of all countries in the world, estimates suggest Ethiopia has the 4th highest number of deaths due to meningitis. Source:www.meningitis.org/mpt, tracking progress tab, IHME estimates for deaths place Ethiopia fourth place.
- Claim: There have been 2,066 cases suspected bacterial meningitis cases reported so far this year. Source:www.meningitis.org/mpt, surveillance tab, Cumulative Cases: 2,066 from weeks 01-17 2022.
- Claim: But global health modellers estimate that there could be more than 100,000 cases of bacterial and viral meningitis per year in the country. Source:www.meningitis.org/mpt, cases and deaths tab, IHME data claiming there were an estimated 116,906 total cases of meningitis in 2019.
- Claim: Estimates suggest there were 320,414 cases of meningitis and neonatal sepsis in 2019. Source:www.meningitis.org/mpt, cases and death tab, IHME data claiming there were an estimated 320,414 cases of meningitis and neonatal sepsis in 2019.
- Claim: Estimates suggest there were 25,196 deaths due to meningitis and neonatal sepsis in one year. Source:www.meningitis.org/mpt, cases and death tab, IHME data claiming there were an estimated 25,196 deaths due to meningitis and neonatal sepsis in 2019.



Mulu’s History

Meningitis Infographics
English



Amharic




Oromo




Key facts
- Meningitis is a devastating disease with a high case fatality rate and leading to serious long-term complications (sequelae).
- Meningitis remains a major global public-health challenge.
- Epidemics of meningitis are seen across the world, particularly in sub-Saharan Africa.
- Many organisms can cause meningitis including bacteria, viruses, fungi, and parasites.
- Bacterial meningitis is of particular concern. Around 1 in 10 people who get this type of meningitis die and 1 in 5 have severe complications.
- Safe affordable vaccines are the most effective way to deliver long-lasting protection.
The focus of this fact sheet is on the four main causes of acute bacterial meningitis:
- Neisseria meningitidis (meningococcus)
- Streptococcus pneumoniae (pneumococcus)
- Haemophilus influenzae
- Streptococcus agalactiae (group B streptococcus)
These bacteria are responsible for more than half of the deaths from meningitis globally and they cause other severe diseases like sepsis and pneumonia.
Other bacteria e.g., Mycobacterium tuberculosis, Salmonella, Listeria, Streptococcus and Staphylococcus, viruses such as enteroviruses and mumps, fungi especially Cryptococcus, and parasites like Amoeba are also important causes of meningitis.
Who is at risk?
Although meningitis affects all ages, young children are most at risk. Newborn babies are at most risk from Group B streptococcus, young children are at higher risk from meningococcus, pneumococcus and Haemophilus influenzae. Adolescents and young adults are at particular risk of meningococcal disease while the elderly are at particular risk of pneumococcal disease.
People all over the world are at risk of meningitis. The highest burden of disease is seen in a region of sub-Saharan Africa, known as the African Meningitis Belt, especially recognised to be at high risk of epidemics of meningococcal but also pneumococcal meningitis.
Higher risk is seen when people are living in close proximity, for example at mass gatherings, in refugee camps, in overcrowded households or in student, military and other occupational settings. Immune deficiencies such as HIV infection or complement deficiency, immunosuppression, and active or passive smoking can also raise the risk of different types of meningitis.
Transmission
The route of transmission varies by organism. Most bacteria that cause meningitis such as meningococcus, pneumococcus and Haemophilus influenzae are carried in the human nose and throat. They spread from person to person by respiratory droplets or throat secretions. Group B streptococcus is often carried in the human gut or vagina and can spread from mother to child around the time of birth.
Carriage of these organisms is usually harmless and helps build up immunity against infection, but the bacteria occasionally invade the body causing meningitis and sepsis.
Signs and symptoms
The incubation period is different for each organism and can range between two and 10 days for bacterial meningitis. Since bacterial meningitis is often accompanied by sepsis, the signs and symptoms cover both conditions.
Signs and symptoms can include:
- severe headache
- stiff or painful neck
- high fever
- avoiding bright light
- drowsy, confused, comatose
- convulsions
- rash
- joint pains
- cold hands and feet
- vomiting
In babies, signs can include:
- poor feeding
- sleepy, difficult to wake, comatose
- irritable, crying when handled
- difficulty breathing, grunting
- fever
- neck rigidity
- bulging soft spot on top of head (fontanelle)
- high pitched cry
- convulsions
- vomiting
- rash
- pale or blotchy skin
Prevention
Preventing meningitis through vaccination is the most effective way to reduce the burden and impact of the disease by delivering long-lasting protection.
Antibiotics are also used to help prevent infection in those at high risk of meningococcal and group B streptococcal disease. Controlling epidemics of meningococcal meningitis relies on both vaccination and antibiotics.
1. Vaccination
Licensed vaccines against meningococcal, pneumococcal and Haemophilus influenzae disease have been available for many years. These bacteria have several different strains (known as serotypes or serogroups) and vaccines are designed to protect against the most harmful strains. Over time, there have been major improvements in strain coverage and vaccine availability, but no universal vaccine against these infections exists.
Meningococcus
The meningococcus has 12 serogroups, with A,B,C,W,X,and Y causing most meningitis.
There are three types of vaccine available:
- Polysaccharide-protein conjugate vaccines (conjugate vaccines) are used in prevention and outbreak response:
- They confer longer-lasting immunity, and also prevent carriage, thereby reducing transmission and leading to herd protection.
- They are effective in protecting children under two years of age.
- Vaccines are available in different formulations:
- monovalent vaccines (serogroup A or C)
- tetravalent vaccines (serogroups A, C, W, Y).
- in combination (serogroup C and Haemophilus influenzae type b)
- Protein based vaccines against serogroup B. These vaccines protect against meningitis in all ages but are not thought to prevent carriage and transmission so do not lead to herd protection.
- Polysaccharide vaccines are safe and effective in children and adults, but weakly protective in infants. Protection is short-lived and they do not lead to herd protection as they do not prevent carriage. They are still used for outbreak control but are being replaced by conjugate vaccines.
Global public health response – elimination of meningococcal A meningitis epidemics in the African meningitis belt
In the African meningitis belt, meningococcus serogroup A accounted for 80–85% of meningitis epidemics before the introduction of a meningococcal A conjugate vaccine through mass preventive campaigns (since 2010) and into routine immunization programmes (since 2016). As of April 2021, 24 of the 26 countries in the meningitis belt have conducted mass preventive campaigns targeting 1-29 year olds (nationwide or in high-risk areas), and half of them have introduced this vaccine into their national routine immunization schedules. Among vaccinated populations, incidence of serogroup A meningitis has declined by more than 99% – no serogroup A case has been confirmed since 2017. Continuing introduction into routine immunization programmes and maintaining high coverage is critical to avoid the resurgence of epidemics.
Cases of meningitis and outbreaks due to other meningococcal serogroups, apart from serogroup B, continue to strike. The roll out of multivalent meningococcal conjugate vaccines is a public health priority to eliminate bacterial meningitis epidemics in the African Meningitis Belt.
Pneumococcus
The pneumococcus has over 97 serotypes, 23 causing most disease.
- Conjugate vaccines are effective from 6 weeks of age at preventing meningitis and other severe pneumococcal infections and are recommended for infants and children up to the age of 5 years, and in some countries for adults aged over 65 years, as well as individuals from certain risk groups. Two different conjugate vaccines are in use that protect against 10 and 13 serotypes. New conjugate vaccines designed to protect against more pneumococcal serotypes are either in development or have been approved for use in adults. Research continues into protein based vaccines.
- A polysaccharide vaccine against 23 serotypes is available but, as for other polysaccharide vaccines, this type of vaccine is considered less effective than conjugate vaccines. It is used mostly in those aged over 65 years to protect against pneumonia, as well as in individuals from certain risk groups. It is not used in children under 2 years of age and is less useful in protecting against meningitis.
Haemophilus influenzae
Haemophilus influenzae has 6 serotypes, serotype b causing most meningitis.
- Conjugate vaccines protect specifically against Haemophilus influenzae serotype b (Hib). They are highly effective in preventing Hib disease and are recommended for routine use in infant vaccine schedules.
Group B streptococcus
Group B streptococcus has 10 serotypes, 1a, 1b, II, III, IV and V causing most disease.
- Conjugate and protein vaccines designed to protect against group B streptococcal disease in mothers and babies are in clinical development.
2. Antibiotics for prevention (chemoprophylaxis)
Meningococcus
Antibiotics for close contacts of those with meningococcal disease, when given promptly, decreases the risk of transmission. Outside the African meningitis belt, chemoprophylaxis is recommended for close contacts within the household. Within the meningitis belt, chemoprophylaxis for close contacts is recommended in non-epidemic situations. Ciprofloxacin is the antibiotic of choice, and ceftriaxone an alternative.
Group B streptococcus
Identifying mothers whose babies are at risk of getting Group B streptococcal disease is recommended in many countries. One way to do this is by universal screening for carriage of Group B streptococcus in pregnancy. Mothers at risk are offered intravenous penicillin during labour to prevent their babies developing Group B streptococcal infection.
Diagnosis
Initial diagnosis of meningitis can be made by clinical examination followed by a lumbar puncture. The bacteria can sometimes be seen in microscopic examinations of the spinal fluid. The diagnosis is supported or confirmed by growing the bacteria from specimens of cerebrospinal fluid or blood, by rapid diagnostic tests or by polymerase chain reaction (PCR). The identification of the serogroups and susceptibility to antibiotics are important to define control measures. Molecular typing and whole genome sequencing identify more differences between strains and inform public health responses.
Treatment
Meningitis is fatal in up to half of patients, when left untreated, and should always be viewed as a medical emergency. Admission to a hospital or health centre is necessary. Isolation of the patient is not usually advised after 24 hours of treatment.
Appropriate antibiotic treatment must be started as soon as possible in bacterial meningitis. Ideally, lumbar puncture should be done first as antibiotics can make it more difficult to grow bacteria from the spinal fluid. However, blood sampling can also help to identify the cause and the priority is to start treatment without delay. A range of antibiotics is used to treat meningitis, including penicillin, ampicillin, and ceftriaxone. During epidemics of meningococcal and pneumococcal meningitis, ceftriaxone is the drug of choice.
Complications and sequelae
One in five people surviving an episode of bacterial meningitis may have long lasting after-effects. These after-effects include hearing loss, seizures, limb weakness, difficulties with vision, speech, language, memory, and communication, as well as scarring and limb amputations after sepsis.
Support and after-care
Meningitis sequelae can have an enormous impact on individuals, families and communities, both financially and emotionally. Sometimes, complications such as deafness, learning impairment or behavioural problems are not recognized by carers and healthcare workers and therefore go untreated.
Those who have lived through meningitis often have health-care needs requiring long-term medical treatments. The ongoing psychosocial impacts of disability from meningitis can have medical, educational, social and human rights-based implications. Despite the high burden of meningitis sequelae on people with meningitis, their families and the community, access to both services and support for these conditions is often insufficient, especially in low and middle income countries. Individuals and families with members disabled by meningitis should be encouraged to seek servies and guidance from local and national Organizations of Disabled People (ODPs) and other disability focused organizations, which can provide vital advice about legal rights, economic opportunities and social engagement to ensure people disabled by meningitis are able to live full and rewarding lives.
Surveillance
Surveillance, from case detection to investigation and laboratory confirmation is essential to the control of meningitis. Main objectives include:
- Detect and confirm outbreaks.
- Monitor the incidence trends, including the distribution and evolution of serogroups and serotypes.
- Estimate the disease burden.
- Monitor the antibiotic resistance profile.
- Monitor the circulation, distribution, and evolution of specific strains (clones).
- Estimate the impact of meningitis control strategies, particularly preventive vaccination programmes.
mostbet kg [url=https://mostbet11025.ru]mostbet kg[/url]
mostbe [url=www.mostbet11022.ru]www.mostbet11022.ru[/url]
Понадобилось найти энциклопедическую статью о Григории Сковороде, и я нашёл её на [url=http://ua-lib.ru/encycl/slovnyk/]сайте Библиотеки украинской литературы[/url]. Статья была не только информативной, но и очень хорошо структурированной. Такой материал полезен не только для учёбы, но и для общего развития.
мостбкт [url=http://mostbet11027.ru/]http://mostbet11027.ru/[/url]
Календарь огородника [url=http://istoriamashin.ru/]http://istoriamashin.ru/[/url] .
Оформиление дипломов ВУЗов в Москве — с печатями, подписями, приложением и возможностью архивной записи (по запросу).
Документ максимально приближен к оригиналу и проходит визуальную проверку.
Мы гарантируем, что в случае проверки документа, подозрений не возникнет.
– Конфиденциально
– Доставка 3–7 дней
– Любая специальность
Уже более 4956 клиентов воспользовались услугой — теперь ваша очередь.
[url=http://poligraf4.ru/]Узнать подробнее[/url] — ответим быстро, без лишних формальностей.
Погода [url=https://inforigin.ru/]inforigin.ru[/url] .
Приобрести документ о получении высшего образования вы можете у нас в Москве. Приобрести диплом ВУЗа по выгодной стоимости возможно, обращаясь к проверенной специализированной фирме. [url=http://cheere.org/create-blog/]cheere.org/create-blog[/url]
Мы предлагаем оформление дипломов ВУЗов в Москве — с печатями, подписями, приложением и возможностью архивной записи (по запросу).
Документ максимально приближен к оригиналу и проходит визуальную проверку.
Мы даем гарантию, что в случае проверки документа, подозрений не возникнет.
– Конфиденциально
– Доставка 3–7 дней
– Любая специальность
Уже более 1101 клиентов воспользовались услугой — теперь ваша очередь.
[url=http://poligraf9.ru/]Купить диплом о среднем профессиональном образовании[/url] — ответим быстро, без лишних формальностей.
Заказать диплом любого ВУЗа!
Мы готовы предложить дипломы психологов, юристов, экономистов и других профессий по доступным ценам— [url=http://kypit-diplom.ru/]kypit-diplom.ru[/url]
Покупка дипломов ВУЗов в Москве — с печатями, подписями, приложением и возможностью архивной записи (по запросу).
Документ максимально приближен к оригиналу и проходит визуальную проверку.
Мы гарантируем, что в случае проверки документа, подозрений не возникнет.
– Конфиденциально
– Доставка 3–7 дней
– Любая специальность
Уже более 1015 клиентов воспользовались услугой — теперь ваша очередь.
[url=http://poligraf5.ru/]На этой странице[/url] — ответим быстро, без лишних формальностей.
iflow домофон [url=https://citadel-trade.ru/]citadel-trade.ru[/url] .
new online casino [url=http://www.maryvaleqld.com.au/new-online-casinos/]http://www.maryvaleqld.com.au/new-online-casinos/[/url] .
mental health app [url=www.mental-health5.com]www.mental-health5.com[/url] .
Гороскоп [url=http://topoland.ru/]http://topoland.ru/[/url] .
Гороскоп [url=https://inforigin.ru/]https://inforigin.ru/[/url] .
казино мостбет скачать [url=mostbet11023.ru]mostbet11023.ru[/url]
australian casinos [url=https://www.maryvaleqld.com.au]https://www.maryvaleqld.com.au[/url] .
официальный сайт mostbet [url=http://mostbet11014.ru/]http://mostbet11014.ru/[/url]
Покупка дипломов ВУЗов по всей России и СНГ — с печатями, подписями, приложением и возможностью архивной записи (по запросу).
Документ максимально приближен к оригиналу и проходит визуальную проверку.
Мы даем гарантию, что в случае проверки документа, подозрений не возникнет.
– Конфиденциально
– Доставка 3–7 дней
– Любая специальность
Уже более 2718 клиентов воспользовались услугой — теперь ваша очередь.
[url=http://poligraf8.ru/]http://poligraf8.ru/[/url] — ответим быстро, без лишних формальностей.
Гороскоп [url=http://istoriamashin.ru/]http://istoriamashin.ru/[/url] .
Пронедра [url=inforigin.ru]inforigin.ru[/url] .
Очиститель сажевого фильтра FLUX «TERMIT»
объемом 5 литров предназначен для эффективной очистки и профилактики выхлопной системы вашего автомобиля. Этот продукт идеально подходит для владельцев дизельных автомобилей, которые хотят поддерживать работоспособность и долговечность своего сажевого фильтра. С его помощью вы сможете предотвратить засорение фильтра, что поможет избежать дорогостоящего ремонта и замены деталей.
[url=https://radikal.host/i/2s0gRv][img]https://e.radikal.host/2025/03/30/to2.md.png[/img][/url]
Формула очистителя
разработана с учетом современных требований, обеспечивая высокую эффективность удаления загрязнений, таких как сажа и копоть, что в свою очередь улучшает работу двигателя и снижает выбросы вредных веществ в атмосферу. Регулярное использование этого продукта позволяет поддерживать оптимальную работу системы и способствует продлению срока службы вашего автомобиля.
[url=https://radikal.host/i/2s09mO][img]https://e.radikal.host/2025/03/30/to1.md.png[/img][/url]
Применение очистителя
Применение очистителя не только безопасно, но и легко. Просто следуйте инструкции на упаковке, и вы сможете быстро и эффективно очистить сажевый фильтр, повышая производительность вашего транспорта. Этот очиститель является отличным выбором для автолюбителей, стремящихся поддерживать свой автомобиль в идеальном состоянии.
[url=https://radikal.host/i/2s0YuE][img]https://e.radikal.host/2025/03/30/to3.md.png[/img][/url]
Купить можно
https://carteams-shop.ru/magazin/product/magazin/product/ochistitelsajevogofiltrafluxtermit
https://www.ozon.ru/product/ochistitel-sazhevogo-filtra-termit-dpf-cleaner-5l-1842332449/
https://www.wildberries.ru/catalog/316931146/detail.aspx?targetUrl=GP
Жидкость для тестирования, калибровки дизельных форсунок и ТНВД «Torch DIESEL SRS»
Специальная жидкость
Специальная жидкость для тестирования, калибровки и консервации топливной аппаратуры дизельных двигателей. Рекомендуется к применению как производителям топливной аппаратуры для ее калибровки и последующей консервации, так и для последующего обслуживания и ремонта на сервисных станциях. Рекомендации по применению SRS Calibration Fluid соответствует ISO-норме 4113 и имеет допуск Daimler-Benz Blatt 133.0.
[url=https://radikal.host/i/2s04Fd][img]https://e.radikal.host/2025/03/30/d1.md.png[/img][/url]
DIESEL TORCH
DIESEL TORCH – обладает следующими преимуществами:
-быстро удаляется с поверхности и не оставляет повреждений
-низкие потери при испарении, за счет узкого диапазона между исходной и конечной точками кипения
-стойкость к окислению
-высокая температура вспышки и высокая диэлектрическая прочность
-хорошие свойства смачивания и промывки
-фильтруется при наличии необходимой системы фильтрации
[url=https://radikal.host/i/2s001I][img]https://e.radikal.host/2025/03/30/d2.md.png[/img][/url]
Купить можно
https://carteams-shop.ru/magazin/product/jidkostdlyatestirovaniyadizelnihforsunok
https://www.ozon.ru/product/zhidkost-dlya-testirovaniya-kalibrovki-dizelnyh-forsunok-i-tnvd-torch-diesel-srs-1842654348/
https://www.wildberries.ru/catalog/317636532/detail.aspx?targetUrl=GP
новости дня [url=www.topoland.ru]www.topoland.ru[/url] .
Приобрести диплом университета. Покупка документа о высшем образовании через надежную компанию дарит ряд преимуществ. Такое решение дает возможность сберечь время и существенные денежные средства. [url=http://orikdok-1v-gorode-volgograd-34.online/]orikdok-1v-gorode-volgograd-34.online[/url]
Следующая страница [url=http://retrocasino.io]newretrocasino[/url]
новые займы 2025 на карту [url=https://vc.ru/niksolovov/2060754-zaim-s-plokhoy-kreditnoy-istoriey-top-17-mfo-2025-goda] новые займы 2025 на карту[/url].
canadian pharmacy cialis 20mg canadian pharmacy no prescription usa no subscription pharmacy pharmacy on line viagra online online pharmacies without scripts healthy man reviews
новости дня [url=www.dorogi34.ru]www.dorogi34.ru[/url] .
мостбет скачат [url=https://mostbet11027.ru/]мостбет скачат[/url]
Магнитные бури [url=http://topoland.ru/]http://topoland.ru/[/url] .
другие https://vodkawin.com/
Какой сегодня праздник [url=https://www.istoriamashin.ru]https://www.istoriamashin.ru[/url] .
Гороскоп [url=http://inforigin.ru]http://inforigin.ru[/url] .
Магнитные бури [url=www.novorjev.ru/]www.novorjev.ru/[/url] .
Лунный календарь [url=www.pechory-online.ru]www.pechory-online.ru[/url] .
История дня [url=http://inforigin.ru/]http://inforigin.ru/[/url] .
скачать мосбет [url=mostbet11024.ru]mostbet11024.ru[/url]
официальный сайт mostbet [url=www.mostbet11026.ru]www.mostbet11026.ru[/url]
Календарь стрижек [url=istoriamashin.ru]istoriamashin.ru[/url] .
Запреты дня [url=www.topoland.ru]www.topoland.ru[/url] .
Гороскоп [url=https://www.inforigin.ru]https://www.inforigin.ru[/url] .
Киного https://kinogoc.top/ фильмы онлайн бесплатно 2025 года!
[url=https://kinogoc.top/]Kinogo[/url]
Гороскоп [url=https://www.topoland.ru]https://www.topoland.ru[/url] .
мосбет скачат [url=mostbet11025.ru]мосбет скачат[/url]
Магнитные бури [url=http://www.istoriamashin.ru]http://www.istoriamashin.ru[/url] .
Календарь огородника [url=www.topoland.ru]www.topoland.ru[/url] .
parimatch android [url=http://parimatch-app-download.com/]parimatch android[/url] .
новости дня [url=https://istoriamashin.ru/]istoriamashin.ru[/url] .
купить диплом в нальчике [url=http://arus-diplom4.ru]купить диплом в нальчике[/url] .
mostbet скачать на андроид официального сайта [url=mostbet11028.ru]mostbet11028.ru[/url]
Вы заказываете диплом в надежной и проверенной компании. Купить диплом о высшем образовании– [url=http://iadvertising.ru/kupit-diplom-menedzhera-s-zaneseniem-v-reestr-bistro-3/]iadvertising.ru/kupit-diplom-menedzhera-s-zaneseniem-v-reestr-bistro-3/[/url]
купить аттестат в оренбурге [url=www.arus-diplom1.ru]купить аттестат в оренбурге[/url] .
mostbet official [url=http://mostbet11026.ru]http://mostbet11026.ru[/url]
Пронедра [url=http://istoriamashin.ru/]http://istoriamashin.ru/[/url] .
sky pharmacy canadian pharmacy
продолжить https://progearph.org/deu/prostatitis/urotonal/
вход мостбет [url=https://mostbet11023.ru/]вход мостбет[/url]
more info here https://saleshophealth.com/lva/vision/product-vizonal/
Покупка дипломов ВУЗов в Москве — с печатями, подписями, приложением и возможностью архивной записи (по запросу).
Документ максимально приближен к оригиналу и проходит визуальную проверку.
Мы гарантируем, что в случае проверки документа, подозрений не возникнет.
– Конфиденциально
– Доставка 3–7 дней
– Любая специальность
Уже более 3828 клиентов воспользовались услугой — теперь ваша очередь.
[url=http://poligraf4.ru/]Посмотреть информацию[/url] — ответим быстро, без лишних формальностей.
Thanks for the article. Here’s more on the topic https://artcet.ru/
Мы предлагаем оформление дипломов ВУЗов в Москве — с печатями, подписями, приложением и возможностью архивной записи (по запросу).
Документ максимально приближен к оригиналу и проходит визуальную проверку.
Мы гарантируем, что в случае проверки документа, подозрений не возникнет.
– Конфиденциально
– Доставка 3–7 дней
– Любая специальность
Уже более 1234 клиентов воспользовались услугой — теперь ваша очередь.
[url=http://poligraf10.ru/]Купить диплом о среднем образовании[/url] — ответим быстро, без лишних формальностей.
use this link https://pharmfriend.net/esp/arthromed/
История дня [url=http://www.novorjev.ru]http://www.novorjev.ru[/url] .
Приобрести диплом ВУЗа по невысокой цене вы сможете, обращаясь к надежной специализированной фирме. Заказать документ института вы сможете в нашей компании. [url=http://orikdok-1v-gorode-cheboksary-21.online/]orikdok-1v-gorode-cheboksary-21.online[/url]
История дня [url=https://pechory-online.ru]https://pechory-online.ru[/url] .
Оформиление дипломов ВУЗов по всей России и СНГ — с печатями, подписями, приложением и возможностью архивной записи (по запросу).
Документ максимально приближен к оригиналу и проходит визуальную проверку.
Мы даем гарантию, что в случае проверки документа, подозрений не возникнет.
– Конфиденциально
– Доставка 3–7 дней
– Любая специальность
Уже более 1988 клиентов воспользовались услугой — теперь ваша очередь.
[url=http://poligraf6.ru/]Пишите[/url] — ответим быстро, без лишних формальностей.
кашпо для цветов высокое пластиковое напольное недорого купить [url=http://kashpo-napolnoe-spb.ru]кашпо для цветов высокое пластиковое напольное недорого купить[/url] .
supreme suppliers india viagra usa online overnight pharmacy
купить диплом государственного образца о высшем образовании [url=www.arus-diplom8.ru]купить диплом государственного образца о высшем образовании[/url] .
pop over to this web-site https://superhealthresources.com/srb/8/eyeon-active/
more https://vitapoint.space/morocco/potency/order-score!-xxl/
сайт мостбет [url=https://www.mostbet11024.ru]сайт мостбет[/url]
1. Вход тут: https://darkstore.cc
2. Вход тут: https://kro34.shop
Официальный сайт: https://captcha-kra34.cc
Кракен маркетплейс является одним из самых популярных и надежных площадок в даркнете, предлагая пользователям широкий ассортимент товаров и услуг. Если вы ищете безопасный и анонимный способ совершать покупки, то Кракен маркетплейс — это отличный выбор. В этой статье мы подробно разберем, как работает площадка, как на нее попасть через официальные ссылки и зеркала, а также какие преимущества она предоставляет.
Для начала работы с Кракен маркетплейс вам понадобится кракен ссылка или кракен зеркало. Поскольку основной домен может быть заблокирован, площадка регулярно обновляет свои зеркала. Официальные ссылки всегда можно найти на darkstore.cc, либо на kro34.shop (в случае блокировки – kro35, kro36 и т.д). Эти домены обеспечивают безопасный вход на Кракен маркет без риска попасть на фишинговый сайт.
Кракен вход осуществляется через специальный переходник, который шифрует соединение и защищает ваши данные. Это особенно важно для тех, кто ценит анонимность. После перехода по кракен ссылка или кракен зеркало вам нужно будет ввести логин и пароль, либо зарегистрироваться, если вы новый пользователь.
Кракен маркет предлагает огромный выбор товаров: от цифровых товаров и документов до электроники и веществ. Площадка работает по системе гарантийных сделок, что минимизирует риск мошенничества. Продавцы проходят верификацию, а отзывы покупателей помогают выбрать надежного поставщика.
Одним из главных преимуществ Кракен маркетплейс является его стабильность. Даже при блокировках основного домена, kro34.shop и другие зеркала позволяют пользователям всегда оставаться на связи. Кроме того, площадка поддерживает различные способы оплаты, включая криптовалюты, что делает транзакции максимально анонимными.
Если у вас возникли проблемы с доступом, попробуйте использовать кракен переходник darkstore.cc или поискать актуальные зеркала на тематических форумах. Важно помнить, что только официальные ссылки, такие как darkstore.cc и kro34.shop гарантируют безопасность.
Кракен маркетплейс продолжает развиваться, предлагая пользователям новые функции и улучшенную защиту. Если вы ищете надежную площадку с большим ассортиментом и высоким уровнем безопасности, то Кракен маркет — это то, что вам нужно. Не забывайте проверять актуальные кракен зеркала и соблюдать правила анонимности для безопасных покупок.
Таким образом, Кракен маркетплейс остается одним из лидеров в своем сегменте, предоставляя пользователям удобный и безопасный способ совершать сделки. Используйте только проверенные kro34.shop домены и следите за обновлениями, чтобы оставаться в курсе новых возможностей площадки.
1. Основной клир для поиска безопасных ссылок, вход: https://darkstore.cc
2. Клир домен Kraken: https://kro34.shop
3. Официальный сайт: https://captcha-kra34.cc
have a peek at this web-site https://zdravsklad.space/germany/milozol/
mostbet ckachat [url=mostbet11029.ru]mostbet11029.ru[/url]
Оформиление дипломов ВУЗов по всей России и СНГ — с печатями, подписями, приложением и возможностью архивной записи (по запросу).
Документ максимально приближен к оригиналу и проходит визуальную проверку.
Мы гарантируем, что в случае проверки документа, подозрений не возникнет.
– Конфиденциально
– Доставка 3–7 дней
– Любая специальность
Уже более 4475 клиентов воспользовались услугой — теперь ваша очередь.
[url=http://inforepetitor10.ru/]http://inforepetitor10.ru/[/url] — ответим быстро, без лишних формальностей.
новые займы без отказа [url=https://vc.ru/dariazah/2060804-onlajn-zajmy-ot-novyh-mfo-top-17-s-minimalnymi-usloviyami-v-2025-godu] новые займы без отказа [/url].
mostbet-download-app-apk.com/ [url=https://mostbet-download-app-apk.com]mostbet-download-app-apk.com/[/url] .
Лунный календарь [url=http://novorjev.ru]http://novorjev.ru[/url] .
internet https://nutramed.health/spain/joints/hondrodox-joint-cream/
купить аттестат в иваново [url=https://www.arus-diplom3.ru]купить аттестат в иваново[/url] .
История дня [url=www.pechory-online.ru]www.pechory-online.ru[/url] .
1. Вход тут: https://darkstore.cc
2. Вход тут: https://kro34.shop
Официальный сайт: https://captcha-kra34.cc
Кракен маркетплейс является одним из самых популярных и надежных площадок в даркнете, предлагая пользователям широкий ассортимент товаров и услуг. Если вы ищете безопасный и анонимный способ совершать покупки, то Кракен маркетплейс — это отличный выбор. В этой статье мы подробно разберем, как работает площадка, как на нее попасть через официальные ссылки и зеркала, а также какие преимущества она предоставляет.
Для начала работы с Кракен маркетплейс вам понадобится кракен ссылка или кракен зеркало. Поскольку основной домен может быть заблокирован, площадка регулярно обновляет свои зеркала. Официальные ссылки всегда можно найти на darkstore.cc, либо на kro34.shop (в случае блокировки – kro35, kro36 и т.д). Эти домены обеспечивают безопасный вход на Кракен маркет без риска попасть на фишинговый сайт.
Кракен вход осуществляется через специальный переходник, который шифрует соединение и защищает ваши данные. Это особенно важно для тех, кто ценит анонимность. После перехода по кракен ссылка или кракен зеркало вам нужно будет ввести логин и пароль, либо зарегистрироваться, если вы новый пользователь.
Кракен маркет предлагает огромный выбор товаров: от цифровых товаров и документов до электроники и веществ. Площадка работает по системе гарантийных сделок, что минимизирует риск мошенничества. Продавцы проходят верификацию, а отзывы покупателей помогают выбрать надежного поставщика.
Одним из главных преимуществ Кракен маркетплейс является его стабильность. Даже при блокировках основного домена, kro34.shop и другие зеркала позволяют пользователям всегда оставаться на связи. Кроме того, площадка поддерживает различные способы оплаты, включая криптовалюты, что делает транзакции максимально анонимными.
Если у вас возникли проблемы с доступом, попробуйте использовать кракен переходник darkstore.cc или поискать актуальные зеркала на тематических форумах. Важно помнить, что только официальные ссылки, такие как darkstore.cc и kro34.shop гарантируют безопасность.
Кракен маркетплейс продолжает развиваться, предлагая пользователям новые функции и улучшенную защиту. Если вы ищете надежную площадку с большим ассортиментом и высоким уровнем безопасности, то Кракен маркет — это то, что вам нужно. Не забывайте проверять актуальные кракен зеркала и соблюдать правила анонимности для безопасных покупок.
Таким образом, Кракен маркетплейс остается одним из лидеров в своем сегменте, предоставляя пользователям удобный и безопасный способ совершать сделки. Используйте только проверенные kro34.shop домены и следите за обновлениями, чтобы оставаться в курсе новых возможностей площадки.
1. Основной клир для поиска безопасных ссылок, вход: https://darkstore.cc
2. Клир домен Kraken: https://kro34.shop
3. Официальный сайт: https://captcha-kra34.cc
Мы предлагаем оформление дипломов ВУЗов в Москве — с печатями, подписями, приложением и возможностью архивной записи (по запросу).
Документ максимально приближен к оригиналу и проходит визуальную проверку.
Мы гарантируем, что в случае проверки документа, подозрений не возникнет.
– Конфиденциально
– Доставка 3–7 дней
– Любая специальность
Уже более 3838 клиентов воспользовались услугой — теперь ваша очередь.
[url=http://poligraf7.ru/]Ознакомиться здесь[/url] — ответим быстро, без лишних формальностей.
Якісний контент, який справді приносить користь. [url=https://xyzdigitalmedia.com/]Це крута команда[/url]!
you can check here https://shopvitality.space/nigeria/vision/visomax/
Где приобрести диплом по актуальной специальности?
Приобрести диплом ВУЗа по выгодной стоимости вы можете, обращаясь к проверенной специализированной компании.: [url=http://diplom45.ru/]diplom45.ru[/url]
Купить диплом на заказ возможно через сайт компании. [url=http://orikdok-1v-gorode-mahachkala-5.online/]orikdok-1v-gorode-mahachkala-5.online[/url]
Заказать диплом о высшем образовании. Приобретение диплома через проверенную и надежную фирму дарит много достоинств для покупателя. Это решение помогает сэкономить время и существенные деньги. [url=http://orikdok-1v-gorode-chelyabinsk-74.online/]orikdok-1v-gorode-chelyabinsk-74.online[/url]
Приобрести диплом института по доступной стоимости возможно, обратившись к надежной специализированной фирме. Мы готовы предложить документы ВУЗов на Ваш выбор, расположенных в любом регионе России. [url=http://momu2.ru/kupit-diplom-s-zaneseniem-v-reestr-bistro-i-nadezhno-4/]momu2.ru/kupit-diplom-s-zaneseniem-v-reestr-bistro-i-nadezhno-4/[/url]
Website https://shopluckyonline.net/revotoxican/
awesome
Мы предлагаем документы ВУЗов, расположенных в любом регионе РФ. Заказать диплом ВУЗа:
[url=http://ractis.ru/forums/index.php?autocom=gallery&req=si&img=3524/]как и где купить аттестат за 11[/url]
[url=https://monolitnyy-fundament-ushp-499.ru]monolitnyy-fundament-ushp-499.ru[/url] .
HAUS IM WALD https://зеленая-жизнь.com/landshaftnoe-proektirovanie/
Перов Вячеслав, 43 https://зеленая-жизнь.com/drenaj/
MR GROUP, ЖК Silhouette https://зеленая-жизнь.com/ozelenenie/
Наши преимущества https://зеленая-жизнь.com/uhod-za-gazonom/
Студия «Агава-М» оказывает услуги ландшафтного дизайна в Москве, Московской Области и всех регионах России с 1996 года https://зеленая-жизнь.com/gazoni/
Гарантия на всё *при нашем уходе https://зеленая-жизнь.com/montazh-gabionov/
Враження від Delta Festival залишаться зі мною надовго. Танцпол «Музична хвиля» був справжнім центром тяжіння завдяки виступам DJ Pendulum і перформансам танцюристів HyperGlow Crew. Неонові вогні і інтерактивні браслети робили кожен момент особливим. Щоб дізнатися більше про цей незабутній досвід, завітайте на [url=https://delta.trancereality.mk.ua/]https://delta.trancereality.mk.ua/[/url].
купить диплом внесенный в реестр [url=https://arus-diplom34.ru/]купить диплом внесенный в реестр[/url] .